• Chronic pelvic pain affects approximately 1/3 of all women and accounts for 15% of gynecology appointments
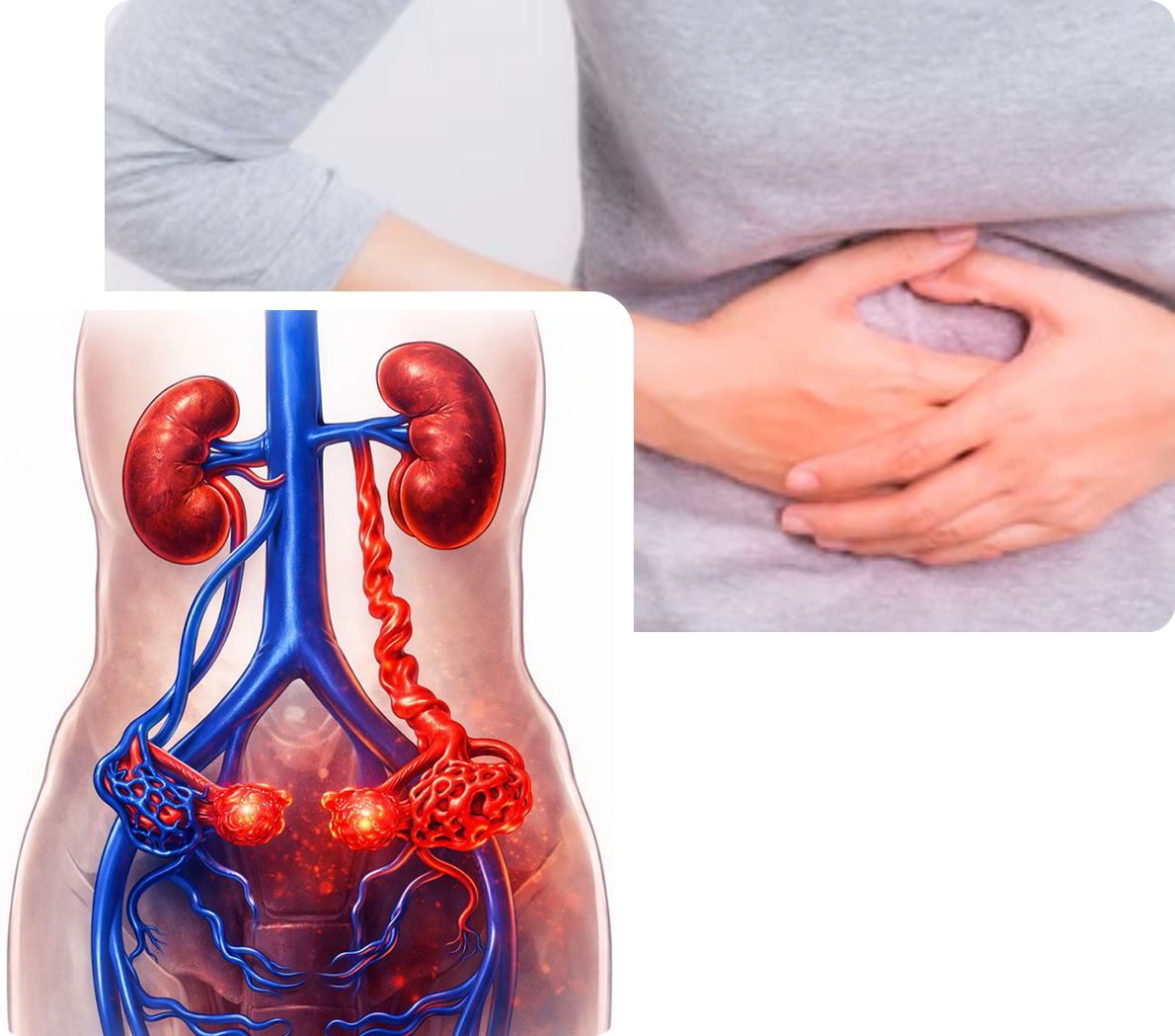
• PCS occurs as a result of damage to valves of the ovarian veins, allowing blood to flow backwards and pool in the pelvis
• Imaging findings of PCS are enlarged ovary veins and resulting varicose veins in the pelvis
• Up to half of all women evaluated for chronic pelvic pain are found to have varicose veins in the pelvis
• PCS is under diagnosed and likely effects about 10% of women
• Symptoms include lower abdominal and pelvic pain and pressure, worsened with standing, menses, exercise, pregnancy, or intercourse
• Hip or leg pain may occur and bulging varicose veins can develop on the vulva and upper legs